

Rhabdomyolysis during training: what it is, why it occurs, and how to reduce the risk
Summary: Rhabdomyolysis is an uncommon but potentially severe condition where muscles break down faster than the body can handle the waste products. The article explains what happens in the muscle and kidneys, why the condition sometimes occurs in connection with training, and which warning signs you should recognize. The main question is how intense physical exertion, heat, hydration status, and energy availability interact—and what you can do to reduce the risk. The conclusion is that rhabdomyolysis rarely affects well-prepared individuals, but knowledge, smart planning, and respect for the body's signals are crucial to avoid serious consequences.
What is Rhabdomyolysis?
Rhabdomyolysis is a condition where the muscles break down for various reasons. The breakdown triggers a cascade of proteins and metabolites that the kidneys need to manage. This can lead to kidney damage if they can't handle the entire cascade, which in turn can become life-threatening.
Rhabdomyolysis was first discovered in the 1908 earthquake that struck Messina, Italy, where survivors often had severe crush injuries from collapsed buildings, resulting in kidney failure due to their muscle injuries.
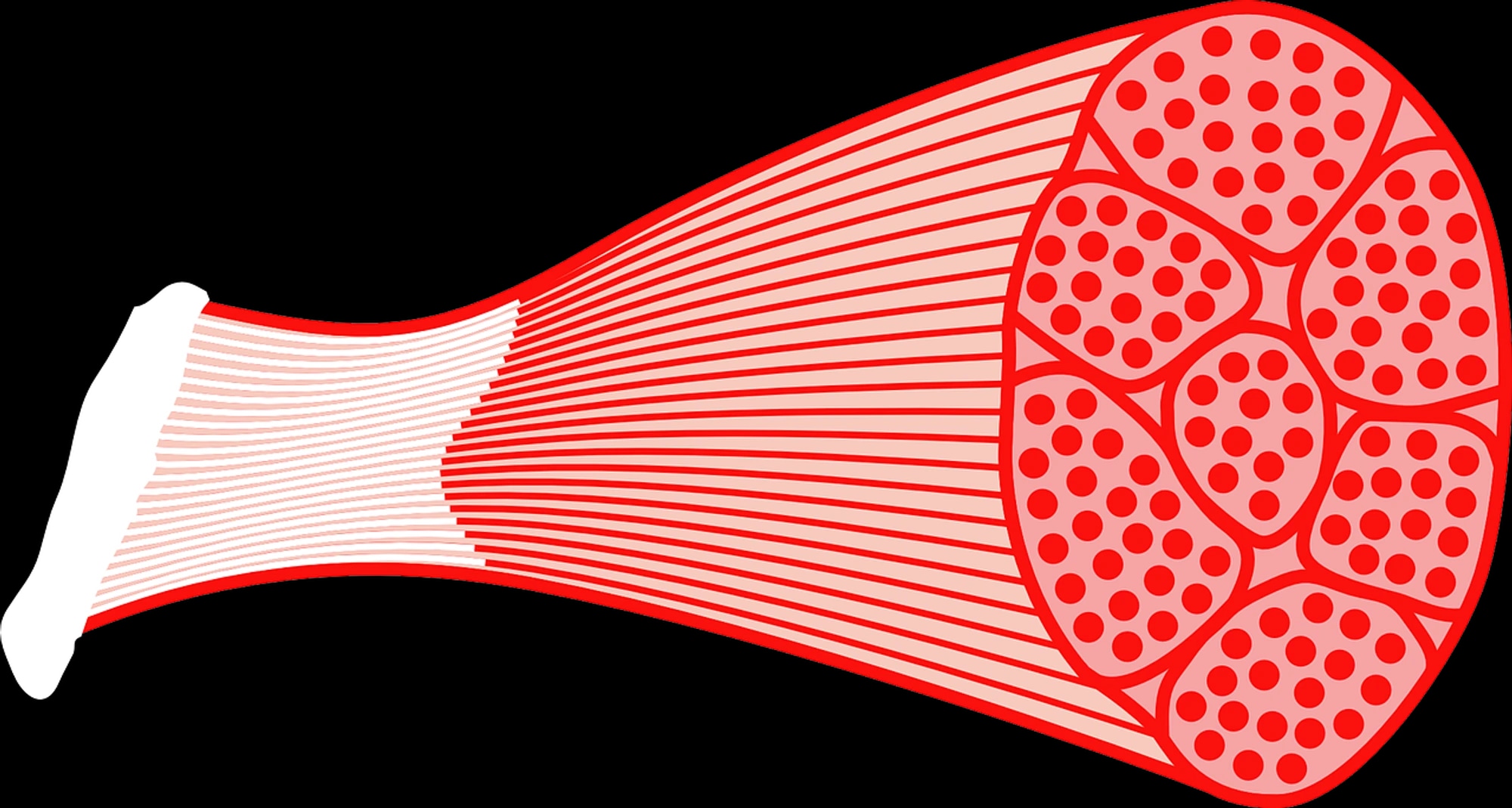
What happens in the muscle?
What's happening is a series of steps where the muscle gets damaged for various reasons. One of the most common factors is crush injuries, but severe illness and being bedridden are also common causes. In the USA, about 26,000 cases per year are reported with symptoms of rhabdomyolysis.
When the integrity of muscle cells is compromised, they lose the ability to produce enough adenosine triphosphate (ATP—the cell's universal energy currency), and the cell membranes lose their function. The sodium/potassium pump, which normally maintains the electrical tension across the membrane by balancing sodium and potassium ions, stops working. This causes sodium to flow into the cell. When sodium rises, the sodium/calcium exchange is also deactivated, meaning the cell can no longer expel calcium as effectively (with a functioning sodium/potassium pump, the sodium/calcium exchange works normally).
If calcium can't be pumped out, various enzymes, including phospholipase A2 (PLA2), are activated, further breaking down the cell membrane. The result is a self-reinforcing breakdown, where even more calcium enters, tissue death occurs, and proteins and metabolites such as myoglobin, creatine kinase (CK), and lactate dehydrogenase leak into the bloodstream.
Small muscle injuries occur all the time, and the body can normally repair them. But when the level of the oxygen-carrying protein myoglobin rapidly increases in the blood (myoglobin normally binds to haptoglobin, like hemoglobin), the kidneys can be negatively affected. With large outflows, haptoglobin cannot bind all the myoglobin, and it is filtered through the kidneys.
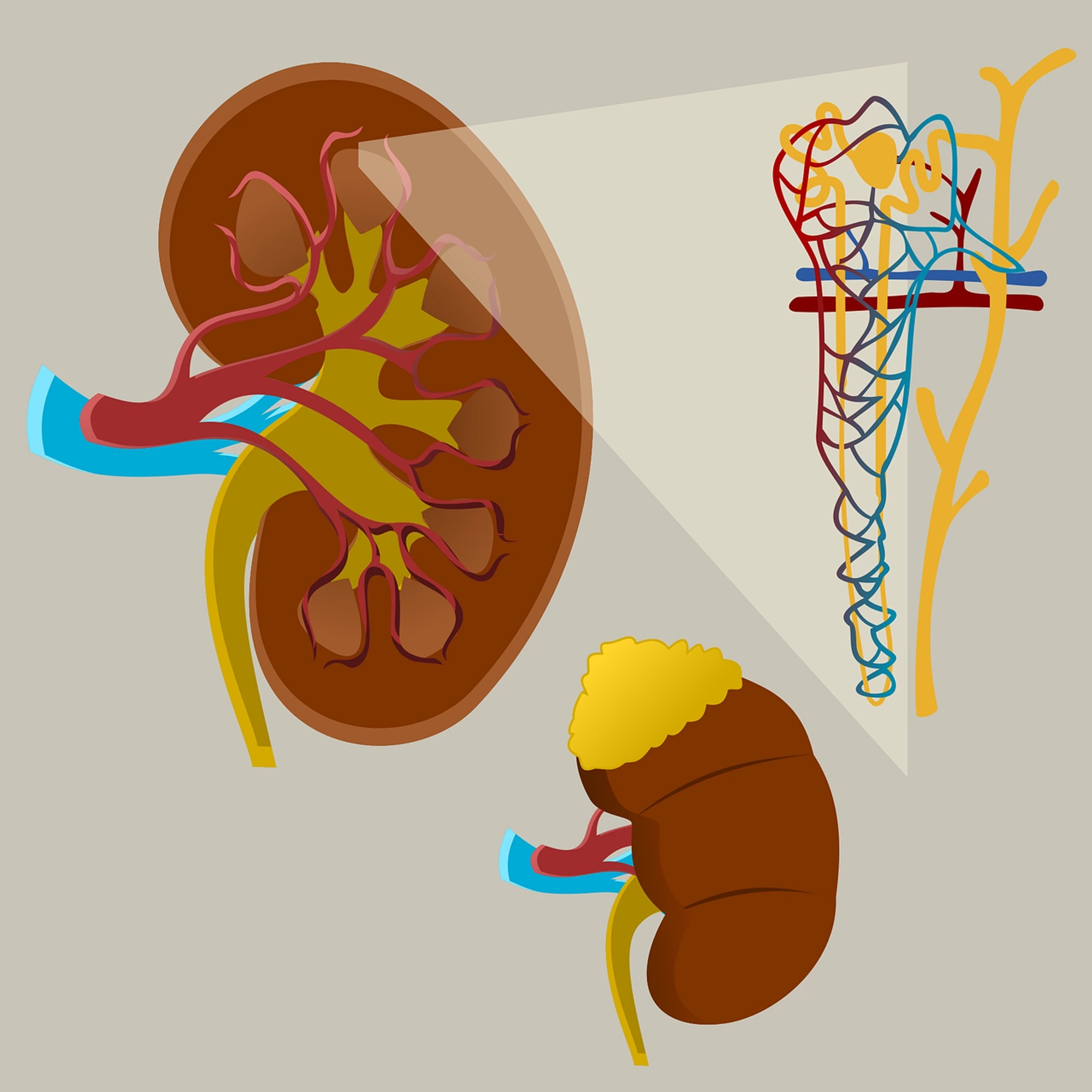
How are the kidneys affected?
The kidneys function as the body's filtration system. Using a series of complex interactions, the body determines if we need to filter out or reabsorb minerals. What's not needed is expelled, leading to urine production. Typically, the kidneys have substantial overcapacity, and we can usually manage with just one kidney with minimal impact on life. However, when high concentrations of myoglobin are filtered through the kidneys, it can cause damage leading to kidney failure.
Myoglobin can form precipitates that block the kidney tubules. The iron released from myoglobin contributes to free radical formation, damaging kidney cells. Combined with an increased uric acid load, it creates a harmful environment for the kidneys, potentially leading to permanent damage if not addressed.
Diagnosis
Diagnosing Rhabdomyolysis involves measuring creatine kinase (CK), reported internationally in international units per liter (IU/L). CK is an enzyme essential for muscles to produce ATP. Its level rises with muscle damage, peaking between 24–72 hours post-injury. Normally, levels range from 45–260 IU/L. In mild Rhabdomyolysis, levels can be five times normal, around 1,000 IU/L, while levels about 5,000 IU/L require follow-up.
Myoglobin measurement is also possible, but it diminishes quickly and may be clinically missed. The classic symptom triad includes muscle pain, muscle weakness, and brown urine. Due to varying hydration status, darker urine can be mistaken for dehydration. Typically, blood myoglobin concentration is about 5.7 nmol/L and urine concentration 0.57 nmol/L. Urine turns brown at concentrations over 57,000 nmol/L. Thus, brown urine indicates significant myoglobin in the blood, but severe rhabdomyolysis can occur without it. Be mindful of other key symptoms like dizziness, nausea, and vomiting.
Why does it happen?
Muscle cells can be damaged by many different causes. Physical stress like crush injuries and repeated muscle contractions, such as long-distance running, are common triggers. Insufficient blood flow to the muscle, as in cramps or epileptic seizures, or prolonged inactivity leading to impaired blood flow can also trigger the condition. Overheating and dehydration make the cells more sensitive and fragile, which further increases the risk.
How can you reduce the risk of developing Rhabdomyolysis?
-
Train for what you plan to do/perform
It goes without saying… Being well-prepared might seem obvious, but it's probably the best advice you can get. Cases where Rhabdomyolysis developed outside of accidents or illnesses can often be traced back to a significant exertion. It could be a 24-hour race or the start of a new training regime/season. Why it occurs sometimes but not in other well-trained individuals is a discussion that will likely never have a 100 percent answer. Summary: if you're competing in downhill running—train for downhill running. The same principle applies to other specific stresses. Do your homework! -
Be recovered but not undertrained
The challenge is to be well-prepared but not exhausted. A classic tip is to maintain frequency and intensity but reduce volume before a race. Keep running regularly at the pace you want to perform at, but shorten the sessions. -
Magic shoes
When you're maximally prepared, make it easier for your body. Shoes with PEBA foam and carbon fiber plates help relieve the muscles. The effect is there even at low intensity. -
Stay well hydrated
A good fluid balance reduces the strain on the kidneys. An early measure when suspecting rhabdomyolysis is to ensure adequate fluid intake to get urine production going. -
Have a solid energy plan
Muscles fueled, especially with carbohydrates, perform better and work at a lower relative intensity compared to exhausted muscles. -
Avoid painkillers especially NSAIDs
They can mask important warning signals such as pain and lead you to continue stressing the body despite warning signs.
Bubblers Also worth mentioning
- Use protein during long events
There’s some research indicating that extra protein during activity can reduce creatine kinase levels after intense training. Research in this area is ongoing, and we are likely to see more interesting studies in the future.
Prospects and Healing
Upon hospital admission, initial treatment begins alongside blood tests: an IV drip. The drip solution often consists of glucose and salt in an isotonic solution (0.9%) to kickstart urine production. The goal is to quickly achieve urine production between 0.2–0.3 dl/h. This increased fluid pressure helps cleanse the kidneys and has proven to be effective in shortening recovery time and improving future prospects.
Recovery time varies with the degree of Rhabdomyolysis. With mild symptoms, often undiagnosed, the kidneys often handle recovery with rest and time. Even more severe cases, where medical help is needed, generally have a better prognosis when the condition arises due to physical exertion compared to causes like illness or trauma (illness and trauma).
General guidelines for returning to training, if tracking creatine kinase levels, suggest waiting until CK values drop to about five times above normal. Then, one can start with light training. This can happen within anything from a few weeks to upwards of 15 weeks. It's important to gradually increase training, avoid overly intense stress initially, and not expose yourself to overheating or dehydration during the rebuilding phase.
Listen to your body, plan smart, and drink moderately—especially when you're aiming for ultra distances. And no, you don't need to fear every muscle ache; but if urine turns dark as coffee and you feel unwell: seek medical attention. We want you back running more ultras, not at the emergency room.